Evidence for simplicity, genericity, openness and holistic competence
N-th mover to Integrated, Person-Centered and Holistic Care
walk the talk, sour grapes, or holistic humbug?
Although, sadly (and all down to me) I stepped off the PhD programme with an MRes, the intention was not to bring my journey with Hodges' model to a close. The joke of course with this model is that you are always presented with a crossroads. As I've written previously (even in draft!) this model is a baton to pass on to others. If the workforce of the 1970s to date evaluates its contribution to health care change and progress, then while the achievements speak for themselves, the challenges* that remain still shout out:- parity of esteem
- integrated - co-ordinated and collaborative care
NHS Innovation Accelerator
Applications for the 2017 NHS Innovation Accelerator (NIA) are now open. For 2017, the NIA is seeking local, national and international innovations that address the following NHS priorities:
· Mental Health
· Urgent and Emergency Care
· Primary Care
The above is now closed but I immediately thought about Hodges' model, given that from the information provided mental health is a priority and a top priority for citizens. Plus, the things that can make a difference to problems:
- Suicide and relapse prevention
- Access and availability with a focus on perinatal, children and young people, dementia and psychological therapies
- Early identification and intervention to minimise the impact on a person’s life, the likelihood of escalation and, in some cases, the chances of survival
- Care closer to home including self-care and access to services at home, in a primary or community setting
- Holistic care of both mental and physical health needs including prevention, screening and treatment for those at greatest risk of poor physical health
"There are many innovations available to improve mental health services, however they are not always used..."
There are however a series of requirements, which present a stumbling block as high impact evidence is lacking.
The purpose of NHS Innovation Accelerator lies in the name. The target is established initiatives and projects that would benefit the NHS and others from a boost of further momentum and leadership support including funding and mentoring. Hodges' model is far from this, but the call is interesting nonetheless.
Reading the details I can argue, for example, that Hodges' model is immediately applicable across the life-span. The model is already designed, but in use the model could be said to meet the requirement of being co-designed with people (including carers, where appropriate). I have used the model with patients and carers (young and adult) who have lived experience of mental illness. With some consideration of the patient, carer, as I have stressed here before on W2tQ the model is accessible to a diverse population. Critically, the delivery of the most significant benefit in terms of outcomes and cost savings needs proof.
It seems that many of the world's problems could be ameliorated through education. This has been evidenced for decades and yet globally there are those who politicise their respective educational system, or even worse deny sections of a society access to education.
In healthcare how can we demonstrate the effectiveness of what is basically a back-of-an-envelope tool? While not a solution Hodges' model helps us to resolve the constituents of healthcare demand and supply, to critically analyse and synthesize - what is going on? I'm sure Hodges' model is just one of many local 'innovations' (in this case created in NW England) that are not evidenced and are therefore missed. Why is this? It may be that the model needs to be re-discovered since being invented somewhere else, by somebody else makes it a non-starter. Similarly, reading the information 'model of care' always grabs my attention:
Your innovation can be a device, digital app or platform,
a service, process, pathway or model of care.
But as is often the case, this is framed in service commissioning, funding, delivery and yes patient outcomes terms. Devices, apps, platforms and services can be specified to a high degree. This is essential to success in research (as is dissemination). Aims and objectives can then be clearly defined, outcomes can be recognised and measured. Processes and pathways are perhaps more fuzzy? These are all important tools, aspects and contexts in health care.
My frustration is that this and similar research formulations seem to exclude tools and resources that are by their nature intentionally simple, holistic, generic and cognitive-reflective. The "model of care" is broken. A whole systems approach# is needed that incorporates education and with it prevention and staying well; plus caring for those affected by illness and disease. We have to honour the legacy problems that the political, education and health systems have 'delivered'. Even if not broken the model of care is missing its twin, the model of life-style choices'.
I still believe there is a model - a conceptual framework - that must precede the (politicised?) model of care, if health and social care are to be truly transformed. Without this, well yes the NHS can accelerate, staff have demonstrated this repeatedly while negotiating all sorts of obstacles. The line of travel will however be circular; circular, but without the discoveries and change gifted to the particle physicists.
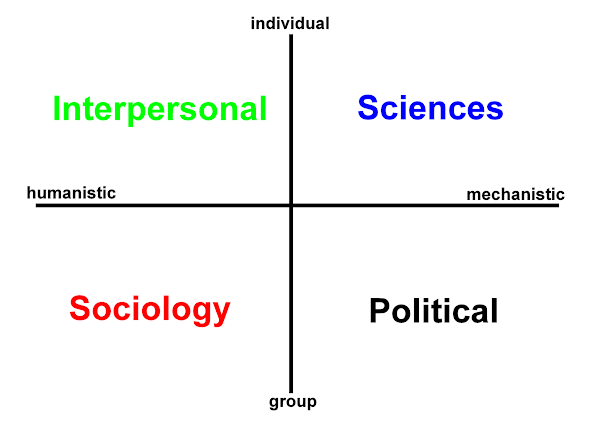
individual
|
INTERPERSONAL : SCIENCES
humanistic ----------------------------------------- mechanistic
SOCIOLOGY : POLITICAL
|
group - population
education mental health cognitive access benefits - outcomes subjective | Evidence process primary care, accident and emergency physical access objective |
qualitative
home
social care
co-design
public engagement
|
quantitative
strategy
'model of care' education system citizens cost savings |
My source:
Irina Johnston
CHAIN Administrative Assistant
If you wish to publicise information on the CHAIN Network please email your request to: enquiries AT chain-network.org.uk
CHAIN - Contact, Help, Advice and Information Network – is an online international network for people working in health and social care. For more information on CHAIN and joining the network please visit website: www.chain-network.org.uk
*
- parity of esteem (a very broad interpretation - the comparison and contrasts between mental health and physical care on several levels - demand, supply, funding, research, integration, staffing, policy, outcomes, evidence-base, social determinants...)
- integrated - co-ordinated and collaborative care (this is not one thing, but several. These terms are sometimes used interchangeably. Care that is truly integrated will also be co-ordinated and collaborative.
![]()

 orcid.org/0000-0002-0192-8965
orcid.org/0000-0002-0192-8965