This 'project' has in reality been ongoing through some thirty years. Although Hodges' model is by its very nature - broad and generic - I'm sure there is a specific research question here. For me this question combines nursing (theory and practice), informatics, health and public engagement. One possible question that h2cm provokes concerns whether the model can be considered a conceptual space?
Over a couple of years I've been adding to some notes which for want of another I've framed under the question above. These notes inevitably languish for a while given a full-time nursing job (plus learning Drupal, this blog, doing posters ...). Picking the text up recently though the intro material seems to have fallen into place. An introduction should cover the recurring issues, challenges - opportunities found in nursing. Although I have the secateurs in hand and the spring is warm, Hodges' model requires that education and cognitive science are also be considered in this way. Anyway, here is the current working outline:
Hodges' model: A mere aide mémoire, or candidate Gärdenforsian conceptual space?
Abstract
Part 1: Introducing Health & Social Care, Education, Hodges' model
1 Introduction
1.1 Health and Social Care
1.2 Recurring Issues in Health and Social Care
2 Education
2.0 Introduction
2.1 Education in the 21st Century
2.2 Issues arising in Education
3 Health Care and Nursing Theory and Hodges' model
3.0 Introduction
3.1 Models of Nursing (Care)
Definitions
3.2 Hodges' Health Career - Care Domains - Model
3.3 Information, energy?, records
Part 2: Cognitive Science & Conceptual Spaces
4 Cognitive Science and Computing
4.0 Introduction
4.1 Models, contexts, situations, the Project and (Darwinian) Justification
4.2 Forms of Literacy, Requirements and Socio-Technical Perspectives
4.3 Computation and Computer Graphics
5 Gardenfors' Conceptual Spaces
5.0 Introduction
Drawing upon the cognitive science and computing literature the objectives of Gärdenfors’ Conceptual Spaces are made clear from the outset:
‘… is to show that a conceptual mode based on geometrical and topological representations deserves at least as much attention in cognitive science as the symbolic and associationistic approaches’ . p.2.
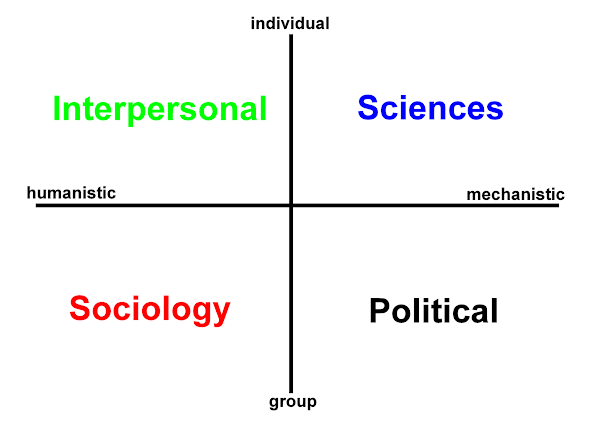
To what extent is h2cm a geometrical and topological representation? It appears on a simplistic level to qualify as a complex plane (Derbyshire, 2008). In this case, however, the closest we get to imaginary numbers in the negative sense are the null hypotheses of clinical research and reasoning amid uncertainty (REF). Gärdenfors continues:
‘This is a book about the geometry of thought. A theory of conceptual spaces will be developed as a particular framework for representing information on the conceptual level.’ p.2.
Hodges' model provides a framework, but as already noted it is not as yet theory based. It is based on practice, with appeals to experience and the knowledge and skills deployed in the health and social care sector. Could the h2cm framework work with Gärdenfors theory of conceptual spaces and his resulting framework for representing information? When Gärdenfors refers to his book being about the geometry of thought, here I would ask: What have nursing theorists sought? In addition to the stated motivations, surely a geometry of nursing thought? Nursing theorists seek rules and laws for a 'geometry' of care. A geometry of care is no less idealised, no less Platonic in form ultimately reflecting the values of the profession. A geometry of care would clearly be an achievement of harmony in the midst of discord and suffering. Additionally as the nursing discipline appears to some to be compromised in respect of practice, training, attitudes and professionalism.
5.1 Representation, Explanation and Construction
5.2 Background on key research methods
5.3 Gärdenfors conceptual spaces - selected definitions
5.4 Purposes, Holistic Bandwidth, Safety, Benefits and the Socio-Technical (repetition, move?)
Part 3:
6 Nursing, Care Theory and Care Domains
6.0 Introduction
6.1 Indicative literature review
6.2 H2CM, Research methods and Data, Data, Data, (Data!)
Conceptual Spaces: Process, Practice and Domains - Hodges’ model
Part 4:
Coding and Classification, Ontologies, RDF, Semantic Web
Icons, glyphs, blobs
Patterns, wholes and parts
Users, Purposes and Scope of Application
Drupal and Ruby
Domains and Domain Specific Languages
Closing Discussion
(Back to this post:)
Don't ask why I am doing this. Chaos does reign here - 'Indicative literature review' in the midst...! In my defence these are notes, what's the question? Bits of the text move about, some disappears. Part 4 could become two, or three new parts, but no more than that! To what extent is there a case for M.I.N.T. a Modern Information-oriented Nursing Theory?*
Can you get there from a conceptual framework? When you get on the "conceptual framework" bus, can we simply change the destination to "conceptual space"? Has the academic bus already been and gone, or it drove right past: "Not in Service". Is this too big an ask of a bus? You need a ship to cross an ocean - even one that is illusory.
One thing I am sure of is that the model - #h2cm, this blog #W2tQ, my picking out Drupal, Ruby and the potential of visualization in the social sciences must come together in some way. One can inform the other. There is something really worth doing here. If in the end I don't get to do it well maybe others can finish the piece (the ambiguity here is intentional). Where's that illusory ship....
* M.I.N.T. sounds better than F.I.H.T. - you know cool and refreshing; but I do prefer and we really do need a Future & Information-oriented Health Theory?
Derbyshire, J. (2008). Unknown Quantity, Atlantic Books. p.12.
Gärdenfors, P. (2000). Conceptual Spaces, Cambridge.




 orcid.org/0000-0002-0192-8965
orcid.org/0000-0002-0192-8965