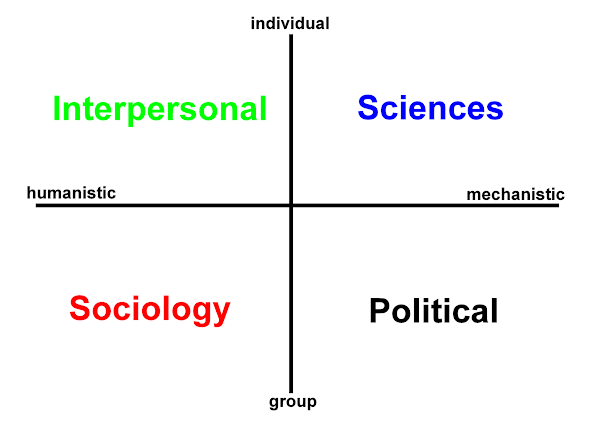
This post extends the axes displayed in the previous post (i) and continues the discussion. These posts are prompted by the appearance of Jeff Jarvis's book - not a reading of it. I suppose they are an ante-review?
As before in the figure I have placed information (and the person) at the center. From (i) - transparency may be a public good in politics, local government and public life, but does the same apply for an individual person? It could be that Jarvis identifies the benefits that can be accrued from being transparent about my medical conditions.
Notable individuals, frequently those already in the public eye, have done so with an activist intent. A key example is
Terry Pratchet with his disclosure and account of living with Alzheimer's disease. Mr Pratchet has been able to raise the public profile of dementia, quality of life in senior years, and also euthanasia and individual choice. If
publicness effects debate in this way then that is clearly desirable. As we have seen with the internet however, there is a market for our data whether personal or merely our internet browsing habits. Where do we go? What are we searching for - a new digital camera, old book, a new HD TV?
Pre-internet a problem for people with condition 'X' or 'Y' was knowing: what to expect? (Even now due to their health and information literacy, a great number of people will still be stuck, excluded and disadvantaged.) What are good strategies to adopt? How have other people coped with this? What happens next? What are the odds? Are there other people living with this? The only opportunities to engage with other people who have something similar may be when sat in the out-patient department. An opportunity a further remove may be the medical diagnostic appointment for various forms of imaging and tests.
These days of course the whole pathway is person-centered and information focused (isn't it?). There are online communities for people living, coping and dealing with the full gamut of clinical disorders, recognized and even some as yet without a place in the medical lexicon.
Part of the debate here for me is that online communities, forums often have rules, they have spam detection and should be 'secure'. Plus of course users are usually encouraged not to use their real name, and be discreet as well as all the other points of etiquette that apply. If Facebook or LinkedIn was to include a new revision that caterred for my 'public' health record then I still wonder if this is publicness of another order. If you assume public office then it is beholden on you to be transparent. It isn't that I believe that transparency on an individual level does not apply. My job has me taking an opaque person and trying to make things transparent.
Perhaps this is the art in health care:
learning to read that which is opaque such that it is rendered transparent?
For all that though I can't help but equate transparency with politics, companies, NGOs and the like.
There's another thing with the
very public health record 4-U; will clinical terminology be affected? This may be a good thing. There are a lot of people, groups who want to shake up the medical establishment, the drug companies and modern practices. Here on W2tQ I wonder about the terms that will be needed in and around Hodges' model. Should a new website use an existing nursing classification, a folksonomy or a combination?
Medical progress has been hard won, many communities around the globe have yet to have access to basic health care, doctors, midwives and nurses. While the developed nations continue to talk about person-centered care, there remain places where ongoing community-centered care would be welcome.
Working in mental health for three decades you know of
psychiatry in dissent and the debates ongoing around stigma, access to services, diagnosis and the use and abuses of medication. I am an idealist in health and informatics, both as distinct
enterprises and in that yet to be fully realised combined formulation.
I worry about the trends in personal information disclosure, the rise of self-diagnosis online, and the growth of
counterfeit drugs sold on the web. Effective and informed self-diagnosis can
save health services time and money, but success, safety, and savings are not a given. So much depends on literacy.
I do hope at some point to read
public parts - it is very timely. We have to ask however, just how far does the market want to reach? Where or what exactly are the envelopes involved? Do we really want to take advertiser's values as one edge of the envelope? If the genie is easy to get back into the bottle then no problem ...
But where do you go to my lovely
When you're alone in your bed
Tell me the thoughts that surround you
I want to look inside your head












 orcid.org/0000-0002-0192-8965
orcid.org/0000-0002-0192-8965