Person centred care, wormholes, pesterers, care domains (i)
Person centred care, wormholes, pesterers, care domains (ii)
Mentor: Shall we re-turn to your question?
Student: OK. Good idea.
Mentor: So to recap how we can define and represent person centered care? Where does person centered care fit in
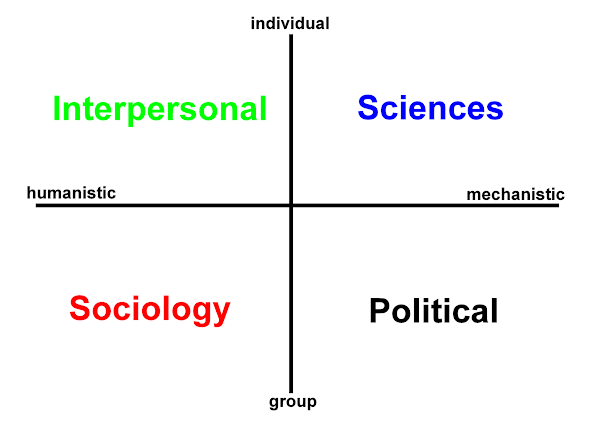
h2cm (Hodges' health career model)?
The INDIVIDUAL-GROUP vertical axis places the person, the individual - at the top of the model. That could be a positive if we are thinking hierarchically, but shouldn't a model that is situated AND person centred be explicit and put the person at the center? Is that the nub of it?
Student: Yes.
Mentor: So can you suggest an avenue to pursue?
Student: No... but I was struck by the talk of movement.
Mentor: And that was your suggestion if I recall correctly. In a similar way you also mentioned ensuring that the individual is taken into account
across all the domains of care. So it sounds like there is a theme there?
Student: Yes, but this may as well be a foreign language - ironically I am stuck - conceptually and physically.
Mentor: Mmm.. What do you do?
Student: Exactly!
Mentor: No sorry, really - what do you do?
Student: I study obviously. Mentor: And...? Student: Well I study and work as a nurse - a student nurse...
Mentor: So you should know the answer? I do not practise clinically as much as I used to, so you have an advantage over me in terms of finding the answer.
Student: If the answer lies in practice?
Mentor: For matters 'person centered' is there a better place to look?
Student: True. OK. So - movement... reasoning...
Mentor: Is your job easy in practice?
Student: It varies of course, but in general - no it's not easy: it takes effort.
Mentor: Ah, now you may have something there!
Student: Oh well that's heartening [with a smile]. In terms of effort then - nursing - health and social care takes concentration and attention as per active listening. You finish a shift and you know you're spent - and there's that assignment and self-directed study to complete.
Mentor: So it sounds like nursing requires - demands even several forms of effort.
Student: Yes in thought and action.
Mentor: And the model - h2cm - can support you in your reasoning and action?
Student: Yes it can because the model encourages you to consider each of the care domains back and forth - and in so doing you move the individual from the top of the I-G axis to the center of the model. Right at the heart, the nexus!
Mentor: So if the model says something about person centered care what does it say?
Student: Well, it says that person centered care is not a given it has to earned. And there - clearly [smiling] is the effort!
Mentor: Well found. Yes, it takes a lot of effort on the part of individual practitioners to put the patient, carer, member of the public - the person - at the center and keep them there. Socio-political factors and lest we forget sometimes the individual themselves will sweep the center clear. What we find and place there are the constraints which are always many and can always be found, such as; location, finance, beliefs, politics... Nursing, health and social care is a constant struggle not necessarily against nature, but with nature and many other factors.
Student: You said something about the INDIVIDUAL-GROUP continuum being irregular and I'm sure there must be more to that?
It's almost as if there are the four pages - the care domains - through which we consider and write our care assessments, plans, evaluations and outcomes. And yet I'm intrigued regards the movement between these pages and the knowledge domains they give rise to.
Mentor: That is another very worthwhile question and in the same way that we remember the fifth care domain - the spiritual; I am sure you will find a way with that question also in good time ...
-+-
 "Riemann's cut, with two sheets are connected together along a line. If we walk around the cut, we stay within the same space. But if we walk through the cut, we pass from one sheet to the next. This is a multiply connected surface."
Kaku, Michio (1994). Hyperspace: A Scientific Odyssey Through Parallel Universes, Time Warps, and the Tenth Dimension. Oxford: Oxford University Press. Fig. 2.4, p. 42.
"Riemann's cut, with two sheets are connected together along a line. If we walk around the cut, we stay within the same space. But if we walk through the cut, we pass from one sheet to the next. This is a multiply connected surface."
Kaku, Michio (1994). Hyperspace: A Scientific Odyssey Through Parallel Universes, Time Warps, and the Tenth Dimension. Oxford: Oxford University Press. Fig. 2.4, p. 42.












 orcid.org/0000-0002-0192-8965
orcid.org/0000-0002-0192-8965
{kind=link}